|
Health Watch
A layman’s guide to bronchial asthma
Tomorrow is World Asthma Day:
Dr.P.N.B.Wijekoon MB.BS.MRCP(U.K.)FRCP (Lond.) FCCP
Consultant Respiratory Physician
Asthma,a potentially fatal disease, has afflicted mankind for
centuries,and,like many other chronic,incurable diseases (asthma is one
of them),the incidence,prevalence,morbidity (ill health and disabilty)
and mortality (death) from asthma has been increasing over the past 40
years,particularly in children.Approximately 300 million people
worldwide suffer from asthma,and its prevalence increases by 50% every
decade.In the United States of America,10% of the population(about 30
million people) suffer from asthma,and the loss to the economy from work
absence, absence from school in the case of children,the cost of
emergency medical care and in- hospital care is astronomical (And Sri
Lanka is no different).
In the United States,for example,10 million school hours were lost
during the course of one year,and,besides having a significant impact on
the quality of education, the consequent loss of productivity for the
parents (when a child is sick one or both parents have stay off work to
care for the child), and the country was U.S.$ One billion (USD
1000,000,000),in one year.The price asthma in adults extracts from the
economy and the healthcare system is incalculable.
Asthma is underdiagnosed and undertreated,leading to unnecessary
morbidity,poor quality of life and avoidable deaths.Approximately
180,000 deaths worldwide are attributable to asthma,and most of these
deaths,especially in young people, could have been avoided if
appropriate,aggressive treatment was instituted early.
Unlike some chronic, incurable diseases like hypertension, diabetes
and chronic kidney disease, which are relatively symptom free until
complications set in, asthma is symptomatic from the start, having a
significant impact on quality of life.
The relentless coughing,wheezing,breathlessness and sleep disturbance
lead to an abyssmal quality of life, resulting in depression,loss of
self esteem and repeated abscences from work or school.
 William Osler (1849 - 1919), Regius Professor of Medicine at Oxford
University, in 1893, defined asthma as a disease of the airways in the
lung characterized by William Osler (1849 - 1919), Regius Professor of Medicine at Oxford
University, in 1893, defined asthma as a disease of the airways in the
lung characterized by
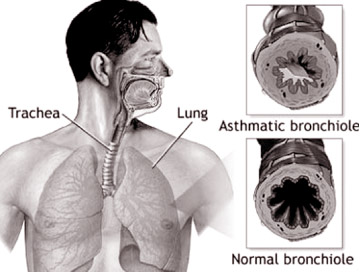
1)Inflammation of the smaller bronchial tubes
2)Hyperaemia (Increased blood supply,redness) and turgescence (swelling)of
the inner lining of the bronchial tubes
3)Spasm of the smooth muscle in the walls of the bronchial tubes and
4)A peculiar exudate of mucin inside the bronchial tubes.
{Explanatory note: Bronchial tubes are the thousands of small,tree like,
branching tubes inside the lung which deliver air from the windpipe
(trachea) to the peripheral lung tissue (alveoli)}.
Osler further goes on to say that “the attacks may be due to direct
irritation of the bronchial mucosa (the inner lining of the air
tubes),or may be induced reflexly,by irritation of the nasal mucosa
(inner lining of the nose ),and indirectly too,by reflex influences from
the stomach, intestines or genital organsÓ(end quote).
How remarkably clever a physician Osler was and how prophetic was his
definition of asthma is exemplified by the currently accepted
description of asthma, which is;
? Asthma - whatever the severity-is a chronic inflammatory disease of
the airways (bronchial tubes) - (Osler said so too.)
? Airway inflammation is associated with airway hyperresponsiveness
(excessive irritability), airflow limitation (less air passing through
the airways), and respiratory symptoms (cough, wheeze, breathlessness).
? Airway inflammation produces four forms of airflow limitation;acute
bronchoconstriction (spasm of the muscle in the air tubes, making them
narrower), swelling of the airway wall, excessive mucus production and
chronic mucus plug formation (Osler said almost exactly the same thing,
120 years ago).
(Source: Global Strategy for Asthma Management and Prevention:
National Heart, Lung and Blood Institute (NHLBI)/World Health
Organization (WHO) workshop report - 2004)
It is indeed remarkable that Osler,more than 120 years ago,without
the help of electron microscopes and bronchoscopes,described asthma
almost exactly as the NHBLI and the world Health Organization describe
it now.Critically,he described chronic inflammation of the bronchi (air
tubes inside the lung),which is now accepted to be the starting point of
asthma and the cause for all its symptoms and long and short term
complications.He went even further than the NHBLI and WHO in describing
the influence of irritation of the nasal mucosa (catarrh),and Gastro-Oesophageal
Reflux Disease (GORD) on exacerbations of asthma,presently accepted as
exerting a significant influence on the asthmatic process.
In fact,in the mid 20th century (1959),asthma was thought to be(quote)
“a disease characterized by widespread narrowing of the airways
(bronchi), which alters in severity either spontaneously or in response
to treatment.” There is no mention at all of inflammation or the
consequences of inflammation - inflammation is now known to be the
foundation of the symptoms, pathophysiology, and the basis for the
present day,rational management of asthma. In the latter part of the
20th century,however, Osler's original definition was found to be
remarkably more accurate,and that narrowing of the airways was a
CONSEQUENCE and not the cause of asthma,the cause being widespread
inflammation of the airways.
Definition
Asthma may be defined,very simply,as “ a chronic inflammatory disease
of the intrapulmonary airways”.For the layman,Óchronic” means lasting a
long time, “inflammatory” means red,swollen and warm, “intrapulmonary”
means within the lung tissue ,and “airways” are the millions of
tiny,branching tubes which carry oxygen from the environment to the
extremities of the lung (the alveoli,which are balloon like structures
where oxygen is exchanged for carbon dioxide (a waste product) in the
blood,and the carbon dioxide is expelled out into the environment via
the same intrapulmonary airways.So,it is clear that the function of the
airways is to supply oxygen (without which survival is not possible) to
the blood,and expel carbon dioxide (a buildup of which is equally fatal)
from the the blood out into the environment.
Because airways resemble cylinders or tubes,according to Pousille's
law,a reduction in the diameter of the cylinder or tube by 50% increases
the resistance to the flow of air by 16 times,and increases the effort
needed to move air in and out of the cylinder or tube by 16 times.In
other words ,a 50% or greater narrowing (as happens in asthma) of the
intrapulmonary airways increases the effort of breathing by 16 times or
more,which is why patients with poorly controlled asthma are so
breathless and exhausted and can even die of the exhaustion.
Because inflammation is the starting point and the sole reason for
the pathophysiology,symptoms,treatment and control of asthma,it is
essential for the layman to have a mental picture of what inflammation
is .A satisfactory analogy is a minor burn on the skin.The affected area
is red (latin;rubor),swollen (tumour),painful (dolor),warm (calor),hypersensitive
(hyperirritable)and loses its function (functio lasae).Exactly the same
thing happens in the asthmatic airway.The affected airway is
red,swollen,warm and it's function(carrying air in and out of the lung)
is impaired because it is narrowed due to the swelling of its inner
lining,spasm of the muscles in its wall,and due to excess mucus
production within.This narrowing of the airway makes it much more
difficult for the patient to breathe because of the tremendously
increased effort (remember Pousille's law),and almost all patients who
die of asthma die of exhaustion and hypoxia (very low levels of oxygen
in the blood inadequate to sustain life),because the airway is too
clogged up and too narrow to carry sufficient oxygen to the alveoli,and
the patient is too exhausted to breathe adequately.This is also why the
first thing a doctor should do for a patient suffering from acute severe
asthma is to administer high concentration oxygen,because prolonged
hypoxia can lead to confusion, coma or death.
Bronchial hyperreactivity
One more, crucially important consequence of airway inflammation is a
phenomenon called bronchial hyperreactivity (syn;hyperresponsiveness,
hyperirritability). The term is self explanatory - when inflamed, the
airways are extremely irritable, and react to substances which would
pass unnoticed by a non- asthmatic individual. This is why asthmatic
patients with poorly controlled asthma react to air conditioning (the
dry, cold air irritates the already irritable airway), or to cigarette
smoke, or to diesel fumes or to viral respiratory tract infections. The
hyperirritable airways react to environmental insults in the only way
they know, which is by narrowing further, swelling further and producing
even more mucus -a protective mechanism, nature's way of preventing the
ingress of the insult further in to the lung.Unfortunately, however,
this protective mechanism worsens the airway obstruction even more.The
predominant symptom of this hyperirritability is a hacking dry cough
(which almost never responds to antibiotics and cough syrups),and often
wheezing.It is important to note that non- asthmatic individuals,too,can
develop temporary bronchial hyperreactivity after a respiratory tract
infection,which explains why many patients come to respiratory
physicians in desperation,because their cough would not go away after
repeated courses of antibiotics (useless in viral infections and which
do absolutely nothing to reduce the inflammation), cough syrups and
diethyl carbamazine,which they have been swallowing ad nauseum.Some are
even treated for tuberculosis,with absolutely no rationale, and without
any clinical,radiological or bacteriological evidence of
tuberculosis.What these patients need is something to control the
ongoing inflammation .It is that simple.
Why are the airways of asthmatic patients so predisposed to
inflammation?The causes are legion-A genetic predisposition (asthma can
be hereditary),gender (asthma is commoner in boys than in girls,though
this difference disappears by age 10),race (asthma incidence is high in
Australia and New Zealand and in black children than in white children
in the United States (though these differences may be attributable more
to socio-economic factors,allergen exposure and dietary factors than a
racial disposition), indoor allergens (e.g;house dust mite, animal
dander, cockroach allergen, rodent allergens and fungi), outdoor
allergens (e.g;pollens,fungi), drugs (e.g;antibiotics, aspirin, certain
pain killers of the NSAID class) , foods (e.g;peanuts, shellfish, milk)
and food additives (e.g; monosodium glutamate, tartrazine). However, it
has to be emphasized that an asthmatic patient may not be predisposed to
any of the above factors,but still develop asthma-many patients in our
clinical practice belong to this category.
Contributory factors
Contributory factors,though they do not actually cause
asthma,increase the likelihood of asthma developing upon exposure to a
causal factor (e.g; house dust mite) in a susceptible
individual.Contributory factors may be active or passive smoking (asthma
is commoner in children in a smoking household than a non-smoking
household), outdoor pollutants (e.g;Sulphr dioxide, ozone,nitrogen
oxide,diesel smoke,dust),indoor pollutants (cooking with natural
gas,liquid propane,kerosene,coal or wood),building or furnishing with
foam installations, glues, fibreboard, pressed board, particle board or
carpet backings.
If inflammation is responsible for all the symptoms,long term
consequences and complications of asthma,it is obvious that the most
logical way of controlling asthma and its symptoms would be to control
the inflammation. And this is indeed so. The present day, logical
management of chronic asthma is based almost entirely on controlling the
underlying inflammation.Control the inflammation,and you control asthma
and its complications.
In the 1950's and 60's, management of asthma was based on relieving
bronchospasm (making the narrowed airways bigger by relieving the spasm
of the muscles in their walls ) with bronchodilators (drugs that relieve
the spasm in the muscles) like Salbutamol.It was later discovered that
long term,regular treatment with bronchodilators actually made asthma
WORSE in the long term,because such treatment did nothing to control the
underlying inflammation.It is akin to applying fresh paint over
rust,without cleaning off the rust (inflammation) first-with time,the
rust (inflammation)breaks out to an even worse extent.Regular treatment
of chronic asthma with solely bronchodilators leads to the patient
requiring larger and larger doses to control the symptoms,because the
underlying inflammation continues unabated and becomes progressively
worse.At some point in time,maximal doses of bronchodilators are unable
to control symptoms,and the underlying inflammation erupts with such
ferocity that the severity of the attack could well kill the patient.
Therefore, the present day management of asthma focuses almost
totally on controlling the chronic airway inflammation.This is the
foundation of adequate treatment and control of asthma-Control of
inflammation rapidly renders the patient asymptomatic,improves quality
of life,prevents sleep disturbance,improves work/school
performance,prevents life threatening complications and prevents long
term damage to the airways,which,if the inflammation is uncontrolled,
can become distorted and permanently narrowed (airway remodelling),and
unresponsive or only partially responsive to any form of treatment,a
condition known as Chronic Obstructive Pulmonary Disease (COPD).
Anti-inflammatory agents
How is the inflammation inside the airways controlled? Obviously,with
anti-inflammatory agents.Though there are many kinds of
anti-inflammatory agents,the most efficacious in the case of asthma are
a class of drugs known as corticosteroids, commonly known as
steroids.Before the reader throws up his hands in horror, let him/her be
reassured that inhaled forms of this class of drug ,because the doses
are so tiny,are safe for long term use.The benefits of inhaled
corticosteroids far outweigh their disadvantages.
They control the ongoing inflammation in the airways rapidly and
effectively because all the symptoms of asthma are due to the underlying
inflammation, the patient rapidly becomes asymptomatic, to such an
extent that he either forgets to continue his medication or erroneously
believes he is cured- a fatal error, because the airway inflammation in
asthma never really goes away, and can last weeks,months,years or
lifelong-inflammation can only be controlled,but not really cured.
Inhaled corticosteroids,if delivered by a correctly used inhaler
device,deliver a tiny dose of the medication to where it is required
-the inflamed airway.
Because it is inhaled and not swallowed,and because the doses are so
tiny (measured in micrograms and not milligrams),very little or hardly
any of the drug gets in to the blood stream,and,consequently ,adverse
effects of the drug on the other organs of the body are minimal or
nil,to such an extent that inhaled corticosteroids are recommended first
line treatment for chronic asthma in children and in pregnancy
complicated by asthma.Typically, one puff from a corticosteroid inhaler
contains only 100 - 250 micrograms of the drug,whereas a single tablet
of Prednisolone (an orally administered corticosteroid tablet)contains
5000 micrograms,though the inhaled dose is far superior to the orally
administered dose.
There are other drugs which complement inhaled corticosteroids and
reduce the requirement for steroids.At the forefront are Long Acting
Bronchodilators (LABD's),which make the narrowed airways bigger and also
possess some anti- inflammatory effect. Long acting bronchodilators are
excellent companions to inhaled corticosteroids,so much so that they are
now almost invariably combined with an inhaled coricostertoid in the
same inhaler device,giving far smoother control of asthma,reducing
exacerbations,improving quality of life and sleep and reducing the
amount of inhaled steroid required.
Unlike in the mid 20th century,short acting bronchodilators like
salbutamol (Relievers) are used only on an as required basis,and not
regularly.In fact,if the patient's asthma is perfectly controlled,he/she
should not require any reliever at all.
Other drugs which complement the above classes of drugs do
exist,useful in difficult to control asthmatics on maximal doses of
inhaled corticosteroids and long and short acting bronchodilators,and in
very mild asthma where inhaled corticosteroids are not
required.Leukotriene receptor modifiers,which block pro-inflammatory
substances called leukotrienes,and drugs belonging to the theophylline
group of drugs are two classes of such drugs.Space does not permit me to
elaborate.
Drugs are NOT the only component in the perfect management of
asthma.Adequate management of asthma has six interrelated parts:
1. Educate patients to develop a partnership in asthma management
2. Assess and monitor asthma severity with both symptom reports
and,as much as possible,measurements of lung function
3. Avoid or control asthma triggers
4. Establish individual medication plans for long term management
5. Establish individual plans for managing exacerbations
6. Provide regular follow up care
Unfortunately,elaborating on the above will likely run in to several
more pages.Suffice it to say that asthma,for so long a cause of untold
misery to millions of patients,can,with appropriate medication,be
controlled (though not cured),to such an extent as to give the patient a
symptom free,near normal quality of life.
This discourse is meant to,as far as possible,provide a clearer
insight into their affliction for the tens of thousands of asthma
sufferers in this country,so that they may be rid of their phobias about
the disease and its treatment,and achieve a quality of life comparable
to that of a normal individual.
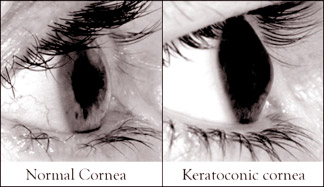
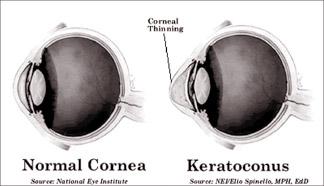
Keratoconus and cross-linking
S Anandarajan - Senior Ophthalmologist
Recently the premier eye hospital in Colombo has introduced this
cross-linking system for keratoconus.
  Many patients and others will be anxious to know what this procedure
is. Many patients and others will be anxious to know what this procedure
is.
The cross-linking is actually a medical procedure that consists of
the use of ultra-violet and riboflavin (vitamin B2).
The aim of this treatment is cross-linking which reduces and stops
keratoconus in the early stages of the condition.
If this condition is thus not prevented it may lead to corneal
transplantation, a major surgical procedure.
Riboflavin is instilled on the cornea and then it is exposed to
ultra-violet light.
This light makes the riboflavin to fluoresce.
This action leads to the formation of bonds between collagen
molecules which are called collagen cross-linking.
This procedure was born in 1998 in Germany.
Now I will describe how the cross-linking is performed.
Anaesthetic eye drops are instilled and the surface cells of the
cornea are gently removed making the riboflavin eye drops penetrate into
the cornea. The drops are allowed to enter into the cornea.
The cornea is then exposed to ultra-violet light.
Today the ultra-violet sources are so advanced making the procedure
time less than an hour. After the procedure a bandage contact lens is
put in and the eye is patched for the night.
New methods are being developed that may allow the outer cells to
remain in place during cross-linking.
Minor complications may occur like pain, sensitivity to light for
many days and blurring of vision will occur for a few weeks. The purpose
of cross-linking is to make the cornea regular allowing soft contact
lenses to be worn without the need for rigid gas permeable lenses. RGP
are good for vision in keratoconus.
Corneal collagen cross-linking with riboflavin is a developing
treatment for keratoconus.
This works by increasing the cross-links of the collagen which are
real anchors within the cornea.
These anchors prevent the cornea from bulging out and becoming steep
and irregular.
This method is not a cure for keratoconus.
This treatment is to arrest progression of keratoconus reducing the
need for keratoplasty. Contact lenses may be needed for following
cross-linking treatment.
This procedure is simple, painless and safe. |







")





