|
Health Watch
Intravenous Pyelogram/ Intravenous Urogram (IVP/IVU)
Dr. Senarath Tennakoon
The IVU is one of the best methods of assessing the pelvicalyceal
system and, until the development of spiral CT and MRI, was the only
satisfactory method for examining the non dilated system. Today non
enhanced spiral CT can be used and is more sensitive. As multidetecter
CT becomes more common, this will likely replace IVU. (McLatchie and
Leaper, 2002).
The principal of an IVP is the administration of a soluble
radio-opaque substance which is filtered by the Glomeruli and excreted
into the urine. The radio-opacity is due to the presence of iodine atoms
and the solution is often referred to as ‘contrast'. Contrast and urine
thus pass down the renal tubles slowly and as water is absorbed from the
loops of Henle and the distal collecting ducts, the number of iodine
atoms per unit volume of urine increases. A radiograph taken at this
stage will demonstrate the position of the kidneys. This is the
nephrogram phase of an IVP. Later contrast and urine reaches the
calyces, pelvis and ureters – the pyelographic phase. An IVP gives the
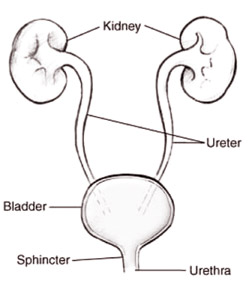
following information:
1. Size, position and symmetry of the kidneys.
2. Anatomy of the renal calyces and renal pelvis
3. The course of each ureter.
4. The size, shape and position of the bladder
Contra-indications to an IVP include sensitivity to organic iodine,
advanced chronic renal failure and the presence of Bence-Jones protein
in urine. Generally and IVP is a very safe investigation and gives a
large amount of information (Gabriel, 1981).
The contrast media used presently are safe but untoward reactions
occasionally occur (Jayakody, 1994) the iodine containing media should
be used with caution in subjects with a known history of
hypersensitivity to iodine; such media interfere with thyroid function
tests. Most contrast media are hypertonic solutions; the side effects
and reactions are higher in patients with combined renal and hepatic
disease. Disorders of water and electrolyte balance should be corrected
before testing and should be monitored even after the procedure (Jayakody,
1994). Urographic and angiographic media are predominantly sodium and/or
methylglucamine (meglumine) salts of benzoic acid. Meglumine salts are
more viscous than sodium salts and are more difficult to inject via
small bore needle. But sodium salts show a higher incidence of side
effects. Most of the conventional contrast media used are of high
osmolality and the side effects are attributed to this feature. So low-osmolar
ionic and non-ionic preparations have been developed for use. Hexabrix
and Hexabrex 320 are ionic low-osmolar contrast media.
The non-ionic low: osmolar contrast media have less side effects
compared to the conventional contrast media and local tissue
tolerability is better(Jayakody,1994). Iohexol (Omnipaque/Omnigraf) is a
tri-iodinated water soluble contrast medium. The extent of protein
binding is minimal and it is excreted unchanged by the kidneys in 24
hours. With intravenous use side effects like sensation of heat,
flushing, nausea, vomiting, itching, urticaria, and chest pain have been
described (Jayakody, 1994). Others are Iopamidol (Iopamino/Niopam
200.300.370) Iopramide (Ultravist) and Metrazamide (Amipaque). The use
of modern contrast agents has made water deprivation unnecessary. In
those with known atopy, diabetes mellitus, or renal insufficiency and
any with a history of adverse reactions to contrast agents, a special
low osmolar contrast medium should be used if the procedure is essential
(Edwards et al 1995).
No other drug should be mixed with the contrast medium being
administered. These should be stored in a cool dry place protected from
light.
How blood groups affect marriages
Dr B G Punchihewa
There are two blood groups systems in humans, namely, the ABO ystme
and the rhesus system.
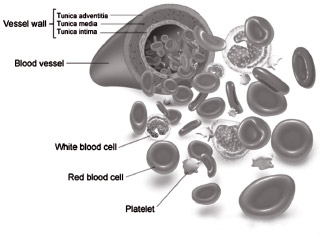
1. In the ABO system, an individual will belong to one of four
groups: A, B, AB and O. A person whose blood group is A, has the antigen
A attached to the cell-surface membrane of his red blood cells (RBC).
A person belonging to the blood group B has the antigen B attached to
the cell-surface membrane of his RBC.
A person belonging to the blood group AB has two antigens (A and B)
attached to the cell-surface membrane of his RBC.
A person whose blood group is O has neither A nor B antigen on the
RBC membrane.
Antigen: An antigen is a protein substance in the body (of a person)
recognized
Chemotherapy is ‘safe during pregnancy’
Jeremy Laurance
Pregnant women with cancer need no longer choose between their own
life and their baby's.

Women diagnosed with cancer during pregnancy no longer need to choose
between their own life and that of their baby. It is possible to save
both.
A series of studies published in The Lancet and Lancet Oncology shows
that children born to women given chemotherapy while they were growing
in the womb developed as well as children in the general population.
About one in 1,000 pregnancies is affected by cancer and in the past
women have faced a terrible choice: delay treatment until the baby is
born, putting their own life at risk, start treatment while pregnant and
risk damaging the baby, or terminate the pregnancy.
Now the trend is to preserve pregnancy wherever possible and the
evidence shows the outcomes for mother and baby are good.
Chemotherapy involves administering toxic drugs to kill the cancer
but which also kill healthy cells in the mother's body. Its effects on
the foetus have been unclear but a study of 68 women who each had three
to four cycles of chemotherapy during pregnancy showed their children
were unaffected.
Tests of cognitive ability on the children were “within normal
ranges”, the researchers from Leuven Cancer Institute in Belgium say.
Only those born prematurely had lower scores of cognitive ability but
the researchers say this applies in the general population too.
“Our findings do not support a strategy of delay in chemotherapy or
[induced] pre-term delivery with [subsequent] chemotherapy to avoid harm
to the foetus,” the authors write.
In a second paper, researchers from the Institut Gustave Roussy say
women must not have chemotherapy in early pregnancy when it can harm the
foetus but from the second trimester (12 weeks) onwards evidence shows
it is safe. “The use of chemotherapy during pregnancy helps increase the
chance of foetal preservation. Children exposed to chemotherapy in utero
after the first trimester do not seem to have more congenital
abnormalities,” the authors say.
However, they admit that women with advanced cervical cancer would
benefit most from a combination of chemotherapy and radiotherapy which
is likely to necessitate termination of the pregnancy.
The authors of a third paper in the series say chemotherapy for
breast cancer can be given in the second and third trimesters and
termination of the pregnancy “does not seem to improve maternal
outcome”. But they add that the decision whether to continue or end the
pregnancy is a personal one.
Case study: ‘Certain drugs don't pass across the placenta. Not
everyone knows that’
Caroline Swain's positive pregnancy test should have brought joy. She
had been trying for a baby with her husband to be a sibling to their
first-born, Max. Instead the result brought terror. Aged 35, she had
taken the test as a precaution, before going into hospital for treatment
for breast cancer, which had just been diagnosed
“I went through all the emotions. Will I live to see my child grow
up? Will I live long enough for him or her to know me? We wanted to save
the baby but the first issue was: would that be possible?”
It was. Caroline's consultant at Southend Hospital in Essex advised
that if she had a mastectomy immediately and waited until she was 12
weeks pregnant to start chemotherapy, her baby should be safe. Luke was
born and is now nine.
“When my consultant told me it was possible to have the baby and the
treatment it was unbelievable. Certain drugs don't pass across the
placenta. Not everyone is aware of that. We are very lucky.”
The Independent
Female hair loss: causes and treatment
Katherine Baldwin
Far from being my crowning glory, my hair has been the bane of my
life. But one question has always plagued me: is my problem on my head,
or in my head? While I've suspected my hair has been thinning for
decades, few people ever believed me and at times I even doubted it
myself.
There were years when my hair seemed fuller, when I'd scrunch it into
ringlets and delight at its apparent thickness. At other times,
particularly in my 30s, I'd fret over the wispy strands at the front of
my head or when I saw too much scalp in the mirror.
My friends always reassured me I had a good head of hair. Most of the
GPs I saw reacted the same, despite my tears and protestations. I had no
bald patches or visible gaps so they'd put it down to stress or would
test my iron and thyroid levels, which appeared normal.
Some of my hair loss over the years is easily explained. I developed
an eating disorder and recall gathering clumps of hair off my pink
bedroom carpet when I was under-eating in my teens.
Weight loss, low iron levels, poor diet and stress, along with
thyroid and hormonal imbalances, can all cause hair to fall,
trichologists say. Hair needs a healthy diet and a well-functioning
endocrine system to flourish.
But diffuse hair shedding linked to weight, anaemia, diet or thyroid
problems is temporary, according to Glenn Lyons, the clinical director
at the Philip Kingsley Trichological Clinic in London. The hair follicle
isn't damaged and the hair grows back automatically or once an imbalance
is addressed.
The same goes for hair loss after childbirth or following cancer
treatment – in most cases hair is restored. Even with alopecia areata,
the sudden hair loss experienced by TV presenter Gail Porter that leaves
bald patches, hair often grows back, although the problem can recur.
There is another type of female hair loss, however, that is less
dramatic and less visible, but can be incredibly distressing. The hair
thins gradually, often over decades, around the top frontal area and
extending back to the crown. It can start at any age, is progressive and
inherited.
“Genetic hair loss is the only hair loss in which the follicle
gradually gets smaller and finer and producers smaller and finer hair
until it stops altogether and then you get the thinning,” says Lyons.
“It has a massive psychological impact on women because they're
balding and thinning in a similar way to the men,” adds Lyons, who sees
women in their teens to their 80s with the condition. “There isn't a
week goes by when we don't get women in tears in here. It affects
self-esteem, confidence, quality of life and relationships.”
Androgenetic alopecia, as the condition is known, is male
hormone-related but isn't caused by too much testosterone. Instead, the
hair follicles become sensitive, due to a genetic predisposition, to
normal levels of male hormones in a woman's body.
But female hair loss is complex and Dr Hugh Rushton, a Harley Street
trichologist, says 72% of women with male hormone-related hair loss are
also iron deficient: “The key is to get an accurate diagnosis and to
eliminate all other potential factors.”
Stress can exacerbate genetic hair loss since the adrenal or stress
glands secrete male hormones into the body, says Lyons. Polycystic
ovaries can also accelerate the condition, and genetic hair loss will
worsen in menopause unless treated as oestrogen levels drop.
- The Guardian
Prize winners in Medical Crossword No. 51
Crossword Coordinator: Edward Arambewala
Following readers who sent entries to the Healthwatch Medical
Crossword No. 51 have won prizes in the crossword draw held on January
27 at the sponsors WISH Institute auditorium, at Delkanda, Nugegoda.
Sponsors are giving gift vouchers of Rs 1,000 each to all winners in
the respective categories, which they can use for eye testing and
purchase of spectacles at special rates. Student category:(1) Entry No.
3 – G K M de Soysa (16 years), St Joseph's Girls School, Gampola. (2) S
Risla (22 years), Kelaniya University. (3) Sadali de Silva (17 years),
Sacred Heart Convent, Galle.
Housewives category:(1) Entry No. 11 - M C S Senn (79 years),
Gangodawila, Nugegoda. (2) Entry No. 3 – S Kutuban (69 years), No. 10,
Palmyrah Avenue, Colombo 3. (3) Entry No. 4 – Duranthi de Croos (59
years), 27, Rukmani Devi Mw., Negombo.
Professionals category:(1) Entry No. 19 – Udaya de Silva (47 years),
teacher, 16/5, Pallewela Road, Gampola. (2) Entry No. 18 – Harshana
Dissanayake (25 years), Business Analyst, No. 22, Jaya Mawatha, Kottawa.
(3) Entry No. 16 – Aresha de Croos (30 years), Data Entry Operator, CCS
Lanka, Colombo.
Pensioners category:(1) Entry No. 4 – W J Cooray (72 years), retired,
16, 1st Lane, Jambugasmulla Road, Nugegoda. (2) Entry No. 8 – Christobel
de Mel (83 years), No. 9, Tickell Road, Colombo 8. (3) Entry No. 9, G L
Wijesinghe (67 years), 578, Gohagoda Road, Katugastota.
Pictures of the prize winners in Crossword No. 50, who received their
prizes at this draw No. 51, next week in this page.
Daily News Editorial with the sponsors WISH Institute congratulates
all the winners
|











")





