Challenges in Leishmania control
Dr Nimal D Kasturiaratchi
 Leishmania
is a communicable disease and comes under the category the Neglected
Tropical Diseases (NTDs). The first patient with Leishmania was
diagnosed by eminent dermatologist Dr D N Atukorala in 1992. The
interests of people aroused by the social marketing campaign of the
leprosy campaign made more people to come to dermatology clinics with
skin patches and that made the diagnosis of Leishmania also possible Leishmania
is a communicable disease and comes under the category the Neglected
Tropical Diseases (NTDs). The first patient with Leishmania was
diagnosed by eminent dermatologist Dr D N Atukorala in 1992. The
interests of people aroused by the social marketing campaign of the
leprosy campaign made more people to come to dermatology clinics with
skin patches and that made the diagnosis of Leishmania also possible
During the last three to four years, about 600 cases in the
Anuradhapura district and about 700 cases in the Matara district have
been diagnosed and treated. However new patients continue to appear and
seek treatment at dermatology units. In a field clinic that was
conducted at Padaviya, Anuradhapura recently consultant dermatologist Dr
Hulangamuwa diagnosed 13 cases of Leishmania that included four
schoolchildren and a teacher from the Padaviya School.
In the North Central Province there are endemic locations such as
Padaviya, Sripura and Thalawa, while in the Southern province Lesihmanis
is found in coastal areas such as Kudawella. In Polonnaruwa too, for
this year, about 25 patients have been detected.
It has not even spared government officers and those who got affected
include PHIs, midwives and Ranaviruvos.
It appears as skin diseases with a non-itching, painless raised dot
in the skin which gets bigger and may lead into a small wound. Some of
the lesions are self-healing. Since the lesions are painless and small
at the beginning most people ignore them and that makes their arrival at
a treatment centre delayed.
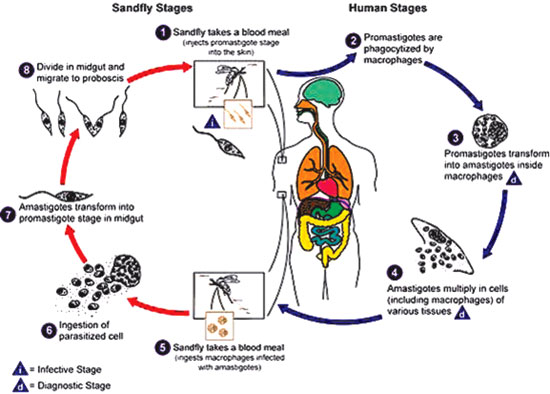
According to medical literature it is a disease spread by sand fly
and is known as a zoonosis meaning humans get it from animals. The
parasite is expected to be harboured in an animal (domestic or wild) and
the sand fly transmits the disease to humans as they bite them.
The skin lesion is usually found at the site of insect bite and
therefore mostly concentrated to the exposed parts of the body. It has
been shown that most commonly lesions are seen in the face and in the
hands.
The sand fly bite is believed to occur from dawn to dusk. But the Sri
Lankan experience shows otherwise and indicates that people are bitten
by this disease-carrying insect even during day. The lifecycle of the
Leishmania parasite has a biological phase within the body of the sand
fly and that has to be completed for the disease to be transmitted to a
human. The Sinhala name for the sand fly is either velimessa or
hohaputuwa.
Leishmania has two manifestations. One as a skin lesion and this type
is called the cutaneous type. However there is a more dangerous type
called the visceral type that affects that makes the liver and spleen to
enlarge.
This type of illness may have fatal consequences and is popularly
known as Kala Azar (‘dark liver’). Kala Azar is found in India (in Bihar
where most of the Buddhist pilgrim sites are located) and in Nepal. The
Kala Azar found in India and Nepal is caused by the same type of
parasite found in Sri Lanka called Donovani Mon 37 . Since its first
diagnosis, some 18 years ago, two patients with Kala Azar have been
diagnosed in Sri Lanka.
Interventions
 |
 |
| Lesion in the
face |
Parasite under
microscope |
Preventing the spread of the disease can be undertaken by minimizing
the people for insect bites. However this is not an easy task. Bed nets,
insect repellents, insecticide spraying and cleaning the household
surroundings are some of the measures that can be adopted. Further
finding the host animal on which the sand flies feed on is also an
important aspect of a prevention program.
However early diagnosis and treatment of patients exposed to this
disease will also help to minimize the risk of human to human transfer
of the disease and the development of complications of the skin lesions.
The skin lesions are treated with injections to the site and also by
clinical burning with liquid nitrogen.
The present experience shows that suspected patients turn up for
treatment rather late. A rough estimate is about four-six months after
observing the skin lesion by an individual for the first time. The
treatment centers are the dermatology units located in government
hospitals and patients may be required to come seven or eight times to
such a clinic for injections and cryotherapy (burning).
A patient in Padaviya loses about one thousand rupees in each visit
in coming to Anuradhapura Hospital for treatment. Approximately, it cost
about ten thousand rupees if they visit Anuradhapura eight times for
treatment. Poor, who do not have such money, may therefore stay away
from treatment. Carrying out field clinics by qualified medical teams
will immensely help these marginalized people to access treatment.
The unknowns and research
There are many unknowns with regard to Leishmania in Sri Lanka. The
primary host is unknown. It could well be domestic animals such as dogs,
cattle, cats or wild animals such as monkeys, rats, birds. Researchers
have found the parasite among a very small sample of domestic dogs. But
they have not demonstrated the parasite within the bodies of sand fly in
Sri Lanka.
It is not yet confirmed that it is the sand fly that is transmitting
the disease in Sri Lanka as attempts to catch the sand fly in the
household of patients have failed.
There is room for more research to be undertaken by the universities
and research institutes. At present the Medical Faculties at Colombo and
Peradeniya are involved in some studies and the Parasitology Department
at the Rajaratara Medical Faculty is teaming up with the Regional
Director of Health Services at Anuradhapura to facilitate the control of
the disease. A similar effort has been initiated at Matara with the
assistance of Galle Medical Faculty researchers.
The transmission from man to man has not been proven but in Sri Lanka
there are instances where more than one member of the family is affected
which could be due to separate insect bites.
There are many challenges in the control of Leishmania. In the
absence of scientific knowledge it will be very difficult to control the
disease-carrying vector (insect) or the primary host (animal). This
leaves us with fewer options. Early diagnosis and treatment will ensure
less suffering to people and prevent the possible complications.
Although field clinics sounds like a good approach, there are
difficulties in drawing upon the human resources from the busy
dermatology units in bigger hospitals.
Similarly both cryotherapy and injections with sodium stibogluconate
are expensive. A vial of 100 mls of stibogluconate costs Rs 18,000.
Sodium Stibogluconate is not a registered drug in Sri Lanka and the
importers have to make special arrangements with the government to
import the drug.
Availability of liquid nitrogen and equipment for cryotherapy are not
easily available in the government sector.
Fairmed Foundation is assisting the health staff in Anuradhapura,
Polonnaruwa and Matara in easing some of these constraints. But more can
be done if more attention is received for this health condition
Danger
Are we posed with a danger? Yes, the present cutaneous can lead into
much more dangerous and costly to manage visceral form with the
appearance of a mutant (genetically modification) of the parasite.
Further it is not known clearly how the cutaneous type can become a
visceral type. But now we have evidence of visceral form already
appearing in Sri Lanka and it is widespread and common in India, Nepal
and Bangladesh.
It could be tomorrow, or within years that we may have a major health
problem in our country and we urge everyone to be aware of this and to
contribute to avert this danger.
The writer is a Medical Social Scientist, Sri Lanka Representative,
Fairmed Foundation
|












")

