|
Healthwatch |
- Compiled and coordinated by
Edward Arambewala |
Obesity: Lifestyle activity vs structured aerobic exercise
Here we give an interesting study conducted by researchers of
obesity, which highlights the importance of active lifestyle. They have
compared a structured aerobic exercise with simple lifestyle activities.
Message it gives...
 There is a very important message this study gives us. That is, a
programme of diet plus lifestyle activity offers similar health benefits
to a programme of diet plus structured aerobic activity for obese women.
It is wise to remember that, lifestyle activities are equally effective
as a method to weight reduction! There is a very important message this study gives us. That is, a
programme of diet plus lifestyle activity offers similar health benefits
to a programme of diet plus structured aerobic activity for obese women.
It is wise to remember that, lifestyle activities are equally effective
as a method to weight reduction!
Study
Participants were 40 obese women with an average age of 43 years,
weight of 89.2kg, height of 165cm and body mass index of 32.9kg/sq metre.
Twenty-eight women were non-Hispanic white, ten were non-Hispanic black
and two were Mexican-American. They were all a minimum of 15kg over
ideal weight and had not participated in a structured exercise programme
for six months before the start of the study. The women were interviewed
to assess their weight, dieting histories, eating and exercise habits,
and psychological status. Anyone with bulimia nervosa, binge eating
disorder, significant depression or other psychiatric disturbances was
excluded from the study. A medical evaluation (performed by their
physicians) identified contra-indications to diet or exercise (e.g.a
recent myocardial infarction or use of medications which would affect
weight or energy expenditure).
The study was a 16-week randomised controlled trial which began in
1995 with one year follow-up. The women agreed not to seek additional
treatment during the one year follow-up period. All the women received a
similar cognitive behavioral weight loss programme of 16 sessions in
which they were instructed in behavioral methods of weight control (e.g.
keeping daily food and physical activity records) and discussed ways of
incorporating physical activity into their lifestyles. All the women
were given the same diet: they were asked to consume a self-selected,
low fat, low calorie diet of approximately 1,200 kcal/day. They were
randomly assigned to either the low fat diet with moderate lifestyle
activity or the low fat diet with structured aerobic exercise.
Lifestyle activity:
The women were advised to increase their levels of moderate-intensity
physical activity by 30 minutes a day on most days of the week;
encouraged to walk instead of drive short distances, take stairs instead
of lifts; and they more monitors to provide information on levels of
physical activity (used to calculate calorie expenditure).
Structured aerobic exercise:
Consisting of three step aerobic classes each week, building up to 45
minutes of stepping per class by the eighth week; total expenditure
approximately 450 to 500 kcal per workout. The following were measured
at the start of the study, at 16 weeks and 68 weeks, by staff unaware of
the women's assigned group:
Weight and body composition: weight, height, and total body fat,
percentage of body fat and fat-free mass, i.e. lean tissue (using whole
body scanner).
Aerobic fitness: maximum oxygen capacity (using a treadmill test),
blood pressure.
Lipids and lipoproteins: blood samples were drawn in the morning
after the women had abstained from food, beverages, or vigorous activity
for 12 hours.
Mood: measured with the Beck Depression Inventory.
Results
Thirty-eight women completed the 16-week trial (nineteen in each
group). Thirty-three completed the 68 week evaluation (16 from lifestyle
group and 17 from aerobic group). Reported energy intake ranged from
1,195 to 1,265 kcal.d during the 16The Observer weeks.
The aerobic group attended an average of 88% of possible exercise
classes.
The lifestyle group had increased their daily physical activity by
234kcal per day by week 16.
Weight loss
Weight losses did not differ significantly between the two groups.
At week 16, average weight losses were 7.9kg lifestyle group and
8.3kg for the aerobic group.
At the one year follow-up, the lifestyle group had regained an
average of 0.08kg and the aerobic group had regained an average of
1.6kg.
Changes in fat and fat-free mass
At week 16, average body fat was reduced by 6.2kg in the lifestyle
group and 7.4kg in the aerobic group.
The percentage of body fat was reduced to 45.5 per cent in the
lifestyle group (from 48.5%) and 41.9 per cent in the aerobic group
(from 46.9)./ Average reductions in fat-free mass were less in the
aerobic group (0.5kg) than the lifestyle group (1.4kg).
Cardiovascular risk factors and mood
At week 16, significant reductions in serum triglyceride levels,
total cholesterol levels and resting systolic blood pressure were found
in all women, with no differences between groups. Significant
improvements in maximum oxygen uptake were also found with no
differences between groups.
Weight maintenance
At the 12 month follow-up there were no difference between the
groups' adherence to physical activity so they were treated as one group
and divided into tertiles of self-reported levels of activity. The most
active group lost weight in the year after the programme (an average of
1.98kg), the middle tertile maintained their weight and the least active
tertile regained some of their lost weight (an average of 4.88kg
increase).
Comment
This was a well designed and carried out trial, albeit small. The
diet plus lifestyle programme was as effective as the diet plus aerobic
training programme in improving weight, systolic blood pressure and
serum lipid and lipoprotein levels.
This is great news for people who dislike vigorous physical activity
or believe that they lack the time to exercise.
The results also show the importance of an active lifestyle in
helping to maintain weight loss. Energy intake will obviously also play
a part.
Details of the women's energy intake at the 12 month follow-up were
not given, but it is likely that the most active group also restricted
their energy intake the most and the least active group restricted it
the least.
Reference
RE Andersen et al. Effects of lifestyle activity vs structured
aerobic exercise in obese women. Journal of the American Medical
Association 1999 281:335-340.
Japanese water therapy
Letter box
I wish to publish my personal' fbs lipid profile' test report records
to draw your attention and hope that it will be of immense help to
provide relief to diabetic patients etc. which does not cost at all.
I am 76 years now and have been bypassed (CABG) 10 years ago and lie
hale and hearty, since the by-pass all my test results were gradually
increasing and on December 24, 2006 glucose level has risen to 135.5 but
instead of using drugs to control it, on the advise of my son who lives
in USA.
I started with 'Japanese water therapy's for six days only and a
lipid profile test was done.
And to my surprise sugar level has come down to 89.1 and with it all
the other levels too have come down by appx 30-40%.
What I did was, early morning before having been a mouth wash tea
etc. I consumed 1 1/2 L. of water (it was difficult at the start but on
my determination, I did it to get over the situation) and now I could
see a great big change, so now I consume 1/2L water in the morning in
addition to water consumed during the day, as before to maintain my
levels and I have found that it works beautifully.
I introduced this 'water therapy to some of my friends and relatives
who had been suffering with diabetic and they have been able to get over
their problems together with other ailments, and are grateful to me.
In addition water therapy is said to cure many other ailments, hence
I sincerely wish to publish this report and my observation so that it
will serve those who are in need.
I do not know why doctors never brief patients about such a valuable
therapy practiced by many world wide?
A.T. Jayalath
Healing Waters
We thank Mrs. Manohari Wickremarachchi BSC (SL) MSC (Bio Med. Sc UK)
MPhil Mol.Bio (UK) for sending us the Nov. issue of - 'Healing Waters'
containing several articles on hydrotherapy on the use of scientifically
prepared water for combating Asthma, Cancer, Dengue, Obesity, Diabetes
and generally for good health.
An interview based article with Mrs. Wickremarachchi on this healing
will be published next week.
Dont forget your Vitamin B12
Dr. D.P. Atukorale
Vegans are vegetarian who do not consume any type of animal products
including milk and honey. A vegan diet rich in fruits, vegetables, whole
grains and legumes provides plenty of protein containing all essential
amino-acids, and an abundance of vitamins and minerals to meet
nutritional needs. You will find plenty of calcium in green leafy
vegetables and legumes. However, there is one nutrient that merits a bit
of planning.
Vitamin B12, which is essential for healthy nerves and healthy blood
in not produced by animals and plants.
It is formed by bacteria and other one - celled organisms.
Animal products commonly contain B12 formed by bacteria in animals
intestinal tracts.
While B12 is also formed in the human intestine, it occurs after the
point where the vitamin can be readily absorbed.
Supplemental Food and B12
Vitamin B12 needs can be met by consuming variety of supplemental
foods, including fortified soy milk, fortified meat analogues, and some
brands of yeast. However, the most convenient and reliable source is a
daily multivitamin. Almost all common brands of multivitamins for
children and adults contain more than enough B12. All vegan adults and
children should take daily multivitamin or B12 supplements of at least 5
micro grams per day. The recommended dietary allowance for adults is 2.4
micro grams per day, with increased requirements for women who are
pregnant or breast feeding.
No case recorded in Sri Lanka
As far as I am aware no case of vitamin B12 deficiency has so far
been recorded among Sri Lankan vegetarians, majority of whom are
lacto-vegetarians and most cases of B12 deficiency have nothing to do
with the diet. People who cannot absorb B12 due to certain diseases or
following certain operations of the gastro-intestinal tract should
regularly take vitamin B12 injections.
Contaminated food and B12
Majority of people in the rural areas, where there is slight
bacterial contamination of the fruits and vegetables, get traces of B12
from the contaminated food. However modern hygiene has eliminated this
source of vitamin B12 and it is always advisable for vegans to take a
multivitamin tablet daily.
Brush your teeth and avoid heart attacks/strokes
Dr. D.P. Atukorala
 It is common knowledge among medical personnel that risk factors for
heart attacks are smoking, high blood cholesterol, diabetes,
hypertension, obesity, lack of exercise, family history of heart attacks
and stress. In addition to common risk factors mentioned above, new
research shows that neglected gums and teeth is another risk factor for
heart attacks. It is common knowledge among medical personnel that risk factors for
heart attacks are smoking, high blood cholesterol, diabetes,
hypertension, obesity, lack of exercise, family history of heart attacks
and stress. In addition to common risk factors mentioned above, new
research shows that neglected gums and teeth is another risk factor for
heart attacks.
According to the World Health Organisation (WHO) heart disease is the
number one killer worldwide claiming about 17 million lives every year
and is the leading cause of death both in the developed countries and
developing countries and in spite of all the precautionary measures
taken by all the governments, the coronary heart disease epidemic is
getting worse.
The WHO now recognises that bacterial infections of the gums and
periodontal infection is an independent risk for heart attacks. In other
words it does not matter how fit and healthy you are, you are adding
your chances of getting heart disease by having bad teeth and bad gums.
There are up to 700 different bacteria in the human mouth and failing
to scrub one's teeth helps those germs to flourish. Most of the germs in
your oral cavity are benign (innocent), some are essential to good
health, but a few can trigger a biological cascade leading to diseases
of the arteries linked to heart attacks and strokes according to new
research by Howard Jenkins of the University of Bristol (UK).
The mouth is the dirtiest place in the human body and mouth is
dirtier than anus, rectum and vulva. According to Steve Kerrigan of the
Royal College of Surgeons in Dublin if you have an open blood vessel
from bleeding gums, bacteria will gain entry to your blood stream and
once inside the blood, the bacteria stick on to certain 'cells' called
platelets causing them to clot inside the coronary vessels and thus
decreasing blood flow to the heart.
Out of the oral bacteria, streptococcus gordanii and Streptococcus
Sanguines are common bacteria that can cause heart attacks according to
Professor Jenkins from the University of Bristol (UK).
It has been shown that gingivitis if treated can lead to
atherosclerosis which, as the readers are aware is the thickening,
tortuosity and build up of fatty plaques within arteries. In about 98%
of patients with heart attacks, primary cause of heart attacks is
atherosclerosis.
A research team headed by Professor Symour, the Dean of the Faculty
of the Dentistry at the University of Otago based their findings on an
analysis of the effect of regular tooth brushing in a group of patients
who were potential candidates for heart attacks. Seymour explained that
a variety of proteins produced by the bacteria initiates atherosclerosis
and helps it to progress. According to world Health Organization (WHO)
neglected teeth can be considered as an independent risk factor for
heart attacks and strokes as mentioned earlier.
Chronic Infection and Coronary Heart Disease
There is scientific evidence to show that chronic infection (e.g.)
periodontal disease could increase the systemic inflammatory response
and directly increase the risk of heart disease and stroke. Major
infectious organisms are Chlamydiae pneumonia, Cytomegalovirus and
Heliobactor pylori. Well-known periodontal pathogens include
orphyromonas gingivalis, Treponema denticola and Actionbacillius.
There is scientific evidence to show that Gram-negative flora
associated with periodontal disease play a significant role in
atherosclerosis and coronary heart disease (angina and heart attacks).
There is also evidence to show that patients with coronary heart disease
(CHD) have significantly increased prevalence of Gram-negative anaerobic
bacteria on tooth surface compared with periodontally healthy reference
group. Dental plaques containing Gram-negative organisms are
significantly higher on individuals who have experienced either unstable
angina or a myocardial infarction just before the dental testing.
Majority of patients with CHD and Gram-negative Organisms tested at
University dental clinics in Michigan University had periodontal
disease.
In the CHD group there was 68 per cent rate of infection
corresponding well with nearly 50 per cent rate of periodontal disease
in patients with acute myocardial infarction (heart attacks).
In two separate case control studies involving 100 patient with acute
myocardial infarction and 102 controls (from the community selected at
random) indices of dental health were significantly worse in patients
with acute myocardial infarction than in controls.
To be continued...
Breast Cancer
For a woman, it is disturbing, even frightening, to find a lump in a
breast. Yet, according to a World Bank report, in 2002 alone, almost
25,000 new and treated cases of cancer were recorded in Sri Lanka,
representing more than a 100 per cent increase over the figures for
1992.
Dr. Shama Fernando heading the Ceylinco Cancer Detection Centre in
Colombo says that breast cancer is generally rampant in women in the
over 50 age group. "High riskers are those in the over 50 age group,"
she said.
A major reason why breast cancer is part of the top list is because
there is more awareness and methods to detect.
"Now more and more women come forward which prompts the statistics to
rise," she says A private healthcare hospital official claims that 8 per
cent reported a physician diagnosis of breast cancer last year at his
hospital and this reflected a 10 per cent increase from the finding of a
methodologically identical survey conducted in 1989.
However the Health Ministry officials reiterate that it is important
to remember that the vast majority of breast lumps are noncancerous
(benign) and that they usually are completely harmless and associated
with a condition called fibrocystic breasts.
They say that nearly 45 per cent of women actually are aware of this
disease and about the same amount visit their doctors to find out.
They say that breast change, causing lumpiness that is more obvious
just before a period, particularly in women over 35.
"Diet also can affect the formation of these uncomfortable lumps and
nodules that usually occur in the upper, outer quadrant of one or both
breasts," Dr. Lansakara says.
Symptoms
Dr. Pawa Palihawadana, Deputy Epidemiologist, Ministry of Health says
that when in doubt what to look out for are
** A lump or thickening in an area of the breast
** A change in the size or shape of a breast
** Dimpling of the skin
** A change in the shape of your nipple, particulary if it turns in,
sinks into the breast or becomes irregular in shape
** A blood-stained discharge from the nipple
** A rash on a nipple or surrounding area
** A swelling or lump in your armpit
Diabetic food pyramid
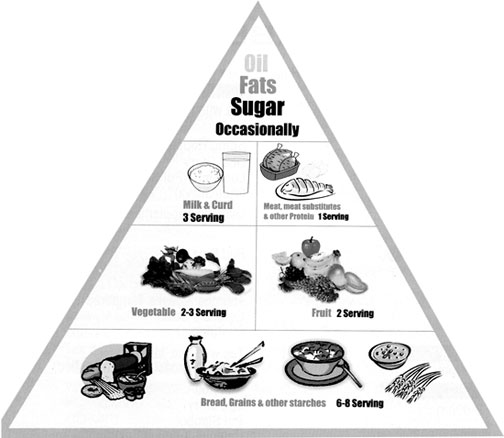
Is a guide to appropriate eating, which divides food into six key
groups of varying sizes.
The largest group grains, beans, rice, starchy vegetables is at the
bottom. This means that more servings of these food should be consumed
more than of any others. Choose a variety of fruits and vegetables
daily.
Choose a diet that is low in saturated fatty acids and cholesterol
and moderated in fat. Choose and prepare foods which are less in salt.
If alcohol beverage is taken, have it in moderation.
Choose food high in fibre, vitamins and minerals such as whole grain,
vegetables and fruits.Be physically active for at least 30 minutes in a
day. |