
|
 |
| Friday, 24 January 2003 |
 |
|
| Features |
| News Business Features Editorial Security Politics World Letters Sports Obituaries
|
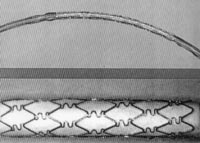
A heart stenting story Health Watch leads today with a "Heart Stenting Story" related to us by Dr. Mohan Rajakaruna, Consultant Cardiologist working in the private sector. Near realisation - 'Drug eluting stent'
In this story Dr. Rajakaruna speaks of a near realization of the much awaited solution to heart blocks (Coronary Artery Disease) - The Drug Eluting Stent - a coil like device coated with a drug which can be placed at the site of the block with a minimum possibility of Restenosis (Reblocking) which heart patients with blocked arteries both here and abroad have been hoping for decades. The most welcome side of the story is for the patients here that though this device "Drug Eluting Stent" is the latest and though expensive is available and could be done in Sri Lanka too without anybody having to go abroad. Bypass; hospital stay; recovery Dr. Rajakaruna explained that in bypass operations to clear heart blocks the chest wall has to be opened up and then the procedure carried out. It is a complicated procedure needing General Anesthesia and the patient has to stay about 7-10 days in the hospital. Some patients even at 1 month do not fully recover. Balloon Catheter - PTCA Researchers were looking for a alternative to bypass surgery and in
1977 developed a balloon catheter which could be inserted from the arm or
leg over a thin wire. This was called Balloon Angioplasty or PTCA. In
this, the expandable balloon is passed to the site of Then the balloon would be taken out. Though this was successful in opening blocked arteries there was a recurrence of the block in about 30-40% (restenosis). In the 1980s cardiologists developed a spring like device called the "stent" which could be placed where the block is. Unlike "Angioplasty" where the balloon is taken out, here the spring which is made of stainless steel is left in place. This enables for a better flow of blood. But yet with the passage of time there was growth of tissue inside the spring. This again lead to the problem of restenosis but was seen only in about 15% - 20%. Drug eluting stent Further research has continued to overcome this problem and in 2001 the "Drug-Eluting stent" had been developed. Many drugs have been used as a coating on the stent but most effective has been an antibiotic called Rapamycin (Sirolimus) and Paclitaxel. These drug eluting stents have reduced the restenosis almost to near zero 5%. In one study the restenosis rate was actually zero! This led to the FDA approving this stent in Nov. 2002. Dr. Rajakaruna said in stenting heart blocks the procedure is simpler, less cumbersome to the patient, General Anesthesia is not given and the patient stay in hospital is one day. Eight patients in drug eluting stent In Sri Lanka he said eight patients have already been stented with the
Drug Eluting Stent and are doing well. Dr. Rajakaruna who has already done
about 700 stent procedures on patients both here and in USA said "The
present indications are that in the future by pass will be a thing of the
past. The stent will bypass the bypass.
T. W. Wikramanayake, Professor Emeritus, University of Peradeniya. The purpose of this article is to draw the attention of the general public as well as health professionals to a document that has, at long last, been published by the Ministry of Health. The task of drawing up dietary guidelines for Sri Lankans was given, in the year 2000, by the Ministry to a Consultative Group of more than forty health professionals, food scientists and nutrition policy planners, who appointed a Working Group of nine persons knowledgeable in human nutrition. Although the Working Group completed their task within 6 months, it was only last week that I received a copy. During the past 50 years the public has been made aware of the need for dietary energy as well as nutrients such as essential amino acids, vitamins, minerals and essential fatty acids and of the quantity of each nutrient that should be consumed daily to maintain good health. Such science-based guidelines were designed to provide guidance on the composition of a healthy diet, and the general public had little information on how much of food available to them should be consumed to provide the requirements of energy and the nutrients. A powerful influence on nutrient intake is food and nutrient availability, which is determined by distribution and utilization of various foods within the population. A fundamental assumption of Food Based Dietary Guidelines (FBDG) is that consumer knowledge will lead to improved food choices and that food availability will reflect these choices. To be effective in bringing about behavioral changes and achieving health goals, the Working Group has made an effort to be practical and has recommended foods that are readily available, accessible and affordable. The government, a regulatory environment, a responsible food industry, the co-operation of health professionals and communicators, all have a vital role to play in achieving the objectives of the FBDG. The government must incorporate the guidelines into a permanent nutrition policy that will remain impervious to temporary changes resulting from political and economic situations. The food industry must develop and support the guidelines by responding to the needs of the consumers (and not their wants). The health professionals should impart the information in the FBDG in a meaningful way. When consumers are informed and educated, they will demand healthier foods. It is hoped that such guidelines will shed light on the confusion created in the minds of the public by opposing recommendations on various foods made by individuals in recent times. Many of these writers rely on information supplied to them by non-scientific publications such as the Readers Digest and publications by individuals or groups promoting sales of particular foods. The public are advised to rely more on information supplied to them by the Medical Research Institute and the Health Education Bureau, both units of the Department of Health Services. Questions could also be referred to the President of the Nutrition Society of Sri Lanka. C/O The Nutrition Unit, MRI, Borella. The Society has among its membership biochemists, physiologists, nutritionists, clinicians and food scientists who could be called upon to express a considered opinion. The FBDG should also be able to solve some problems. For instance a recent recommendation by a cosmetic surgeon that one should consume 1000g fish oil daily would not have been made had he been aware that 1 gramme of a fat or oil supplies nine kilocalories and that the recommended energy intake for all persons is well below 3000 kilocalories. His prescription, if adhered to, will make us a very obese population! It is also hoped that these guidelines will be made available to the general public in all three national languages and in the form of posters, brochures and radio and television messages. Educational materials containing explanations and specific information on serving portions for traditional as well as packaged foods, compared with homemade foods, should supplement the FBDG. Lastly, these guidelines should be reviewed periodically, say once in every five years, in keeping with advances in the knowledge of the physiology and biochemistry nutritional science. The Focal Point for the FBDG is stated as the Director, Nutrition,
Department of Health Services.
Prof. Nalaka Mendis, the Head of 'Sahanaya' in an interview with Health Watch last week revealed that 'Sahanaya' is planning to expand its education rehabilitation and mental care services this year by setting up a new service centre in Bolgoda, Moratuwa, land donated by a well-wisher. The National Council for Mental Health - 'Sahanaya' was instituted in 1983 with the general objective of promoting ways and means for social rehabilitation of persons who have suffered mental illness. This non governmental organization has established a mental health centre to carry out mental health care programmes for the community. The activities of the centre have grown over the years and at present it offers clinical, rehabilitation, public education, training and other special services. Its operations are funded mainly with the interest on investments, and donations. A significant proportion of the activities is carried out on a voluntary basis by professionals and other volunteers. Sahanaya to expand With the increase in demand for such services and the lack of investment in this area by the state, 'Sahanaya' now proposes to expand its activities by setting up a Centre for Mental Health and Psychosocial Care to provide services for those with mental health problems, families, care givers, professionals and the community. The Primary focus will be on disabled, distressed, traumatized, suicidal and those with other types of mental health problems. The key objective of the expansion will be to provide a series of services, which are not presently available in the State sector mental health care thus widening the range of services available to people with mental health problems, which will undoubtedly strengthen the mental health care in the country. It will focus on expanding clinical care and counselling programmes, carrying out information and education programmes, training and engaging in special projects including research, pilot projects and advocacy activities to cover the needs of the above people. The proposed programmes will be developed by a core group of professionals and an attempt will be made to integrate these services to existing services. An attempt will be made to mobilize and coordinate the resources of the family, community and the existing care agencies to address problems in a holistic manner. Apart from day programmes the centre will provide hostel facilities for clients as well as groups undergoing training including care givers. The outreach programme will initiate community activities both in clinical and rehabilitation areas. In order to promote sustainability and institutional development attempts will be made to integrate some of these services to existing community and institutional structures over time. This will involve development of not only new services but new management approaches and policy development. The clinical programme is expected to serve about 6,000 persons annually. The rehabilitation programme consisting of residential and out-patient facilities will cater to about forty persons at a time. The information centre apart from developing educational material will carry out a public education programme. The training programmes will conduct mental health and psychosocial care program both residential and day basis to twenty five persons monthly. The family education programmes will conduct residential training twice monthly for 15 persons at each time. New site at Moratuwa The proposed site, donated by a well-wisher is located at Moratuwa - Gorakana by the Bologoda Lake, provides a tranquil environment for the project. The architectural concept in designing the proposed facility takes into account the need to preserve the serenity of the environment, conducive to the rehabilitation of the mentally disturbed. The area of the proposed building is 29,467 square feet and was conceived and designed by architect Terner Wickramasinghe. The Total project cost is estimated at Rs. 131,835,000. The details are as follows: It is proposed to cover a portion of the operational expenditure of the centre through the fees charged from patients, and through donations. The balance portion is expected to be raised through the interest income earned on the proposed capital reserve. If there are constraints to raise the total capital requirement at once, it is proposed to carry out the project in two phases. A board of trustees comprising of seven persons with wide experience in the fields of Investment, Management, Administration, Accounting, Law and Banking will be appointed to be in charge of investing funds and generating new funds for the activities of the organization. The funds raised for the building project will be administered by a committee comprising of leaders from the business community who have already taken a lead role in setting up the fund and a representative from the management committee. The implementation of the project will be carefully monitored by a steering committee to ensure smooth delivery on schedule within the stipulated costs. This committee will comprise of experts in construction and finance and will communicate the progress of the project implementation to the donors, regularly. Mental and behaviourial disorders constitute more than twelve percent of Global Burden of disease. More than ten percent of people suffer from mental disorders at any given time. In Sri Lanka the mental and behavioural problems are not only serious problem at present but are likely to increase especially in vulnerable groups such as women, children, elderly, traumatized, displaced, disabled and impact even more in quality and quantity in the coming decades. More than half of the people committing suicide are likely to be suffering from a mental disorder. Nearly five thousand people are likely to suffer from serious mental disorders such as schizophrenia, mood disorders, dementia, child disorders, alcohol problems and mental retardation. A much higher proportion of people suffer from a range of other disorders due to stress, trauma, displacement and various forms of deprivation. Hospital statistics show a marked increase in utilization of the mental health facilities. The response of the community to this enormous human suffering is
marginal at its best. There is very little discussion, awareness, concern
and sympathy among public on mental health issues. Mental health has not
been included in any list of priorities apart from being identified as
tokenism by the government and other state agencies including the ministry
of health. The ministry spends less than 1.5 per cent of the health budget
on mental health which is less than half that was allocated thirty years
ago.
Walking for health and fitness Pace-walking, or walking for fitness, is a natural and simple way of exercising to improve our heart and lung function, circulation, and to tone our muscles. Being a low impact activity, it is safe for people of all ages and fitness levels as there is very little risk for injury. It is a stepping stone to other more vigorous forms of activities. What to wear * Use sports or PT shoes which are light, flexible, well-padded, well-fitting with proper arch and heel supports. If socks are worn, they should be short socks. * Wear loose, light, porous, short-sleeved T-shirts and shorts. These will ensure comfort and minimise fatigue and injuries. How to walk * Look ahead * Breathe naturally through mouth or nose * Back erect * Arms slightly bent, swing naturally * Stomach and buttocks pulled in * Heel to toe landing Stable and smooth paths are best. Avoid rough and uneven or sloping surfaces which keep you off-balance and may cause injury. Try to choose a course that avoids heavy traffic and pollutants. If you pace-walk on the roads, always walk facing oncoming traffic and observe traffic rules. When walking in the dark, wear light-coloured attire preferably with luminous reflectors so that motorists can see you better. As a beginner, expect some stiffness, aches and pains in the leg muscles. Often, pain which persists in the toes or ankles, or in the knee joints, hips or lower back are a result of poor shoe support. Pains in calf or thigh muscles often result from over-use of the muscles. These conditions should clear in a few days with continued modified walking; otherwise you should see a doctor. some general precautions to observe * Do not go on an exercise programme without first consulting your doctor if you have significant medical problems, are above 35 years of age, have been inactive or are not certain of your health or fitness level. * Do not do too much too soon. Stay within your own capabilities, but at a sufficient intensity to get results. * Do not engage in any vigorous exercise 2-3 hours after a meal. * Do not exercise when feeling unwell or when suffering from a significant injury or acute infection. Resume only when you have fully recovered and gradually build up to your previous intensity. How often, how hard, how long To get best results, you should develop a proper exercise programme which incorporates the principles in the "FITT" formula: Frequency: 3-5 times a week (a regular, consistent schedule is important) Intensity: Exercise until you begin to sweat and breathe deeply without feeling discomfort or at an intensity of 60%-85% of your predicted maximum heart rate (MHR). To calculate the MHR, minus your age from 220. Type Callisthenic (e.g. stretching exercises) and aerobic exercises (e.g. brisk walking, jogging, swimming) Time or duration: Each workout session should comprise 3 phases: * warm up callisthenic exercises (3-5 minutes) * aerobic exercises (15-60 minutes) * cool down callisthenic exercises (3-5 minutes) * If you are a beginner, start off with the following programme: Level 1: Pace-walk 15-30 minutes 3-5 times a week or 15-20 minutes 6-7 times a week Level 2: Pace-walk 30-45 minutes 3-5 times a week or 20-30 minutes 6-7 times a week. Level 3: Pace-walk 45-60 minutes 3-5 times a week or 30-45 minutes 6-7 times a week. Level 4: Pace-walk at least 60 minutes 5-7 times a week. The materials in this pamphlet are extracted from the following sources: * Sports Medicine Exercise and Fitness: A Guide for Everyone by Dr. C. K. Giam and Dr. K. C. Teh, PG Publishing, 1988. * Being Fit: A Personal Guide by Bud Getchell and Wayne Anderson, John Wiley and Sons Inc, 1982. * Jogging Your Way to Health and Fitness by James Hewitt, New English
Library Limited, 1988. Sent by T. Perinpanayagam ex-DIG, Traffic, Colombo
6
Last week Sri Lanka's oldest centenarian 115 year old Engonona got a new year gift pack of consumer items from Lever Brothers Ceylon Ltd. A representative from Levers Personnel Department travelled down to Galle to handover the gift pack and convey the company's new year greetings to her. Levers are looking into the possibility of donating monthly needs of Lever consumer items to her for the rest of her life. Also present at the occasion was Siri Gunasekera a Sri Lankan living in New Zealand, who is also from Unawatuna, Galle. Mr. Gunasekera who is popularising 'Anapanasathi' Buddhist meditation both in New Zealand and Sri Lanka, had read about Engonona in the Daily News internet edition had been looking forward to visit her this time when he makes his annual visit to Sri Lanka. He has also undertaken to get help from New Zealand to Engonona and also for the Colvin Gooneratne Centenarian Study Project. He has also joined the Centenarian Friendship Association headed by Prof. Goonaratne, to promote the cause of living Centenarians in this country.
UK study on racism and disease Studies in the United States report associations between perceived racial discrimination and high blood pressure, birth weight, and days off sick. In a recent study from the United Kingdom, victims of discrimination were more likely to have respiratory illness, high blood pressure, anxiety, depression and psychosis. Stress responses have been considered possible mechanisms for the effects of racism on health. Considering racism as a cause of ill health is an important step in developing the research agenda and response from health services, says the author. Yet despite general agreement that racism is wrong, there is little evidence of any concerted and effective initiatives to decrease its prevalence. This means that in the United Kingdom the science of investigating the effects of racism on health and the development of preventive strategies are in their infancy. How can we have equity in health if one of the major possible causes of illnes in minority ethnic groups in the United Kingdom does not have a dedicated research effort or prevention strategy? he concludes. (From the BMJ Jan. 9 issue sent to Health Watch by Dr. Dennis J. Aloysius) |
|
News | Business | Features
| Editorial | Security
Produced by Lake House |

 blockage and then
inflated (blown up). The balloon "opens up" the blockage by
compressing the plaque and stretching the artery open. (It is much like
stretching open the elastic part of a sock with your hands).
blockage and then
inflated (blown up). The balloon "opens up" the blockage by
compressing the plaque and stretching the artery open. (It is much like
stretching open the elastic part of a sock with your hands).



