|
Health Watch
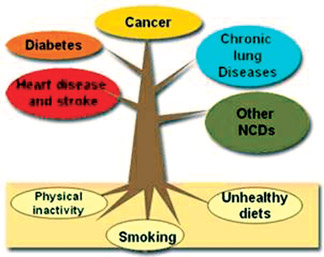
What causes non-communicable diseases?
Manjari PEIRIS
Non-communicable diseases (NCDs) are the leading causes of death
globally, killing more people each year than all other causes combined.
Contrary to popular opinion, available data demonstrate that nearly 80
percent of NCD deaths occur in low and middle-income countries. Despite
their rapid growth and inequitable distribution, much of the human and
social impact caused each year by NCD-related deaths could be averted
through well-understood, cost-effective and feasible interventions.
 Of
the 57 million deaths that occurred globally in 2008, 36 million –
almost two thirds – were due to NCDs, comprising mainly cardiovascular
diseases, cancers, diabetes and chronic lung diseases. The combined
burden of these diseases is rising fastest among lower-income countries,
populations and communities, where they impose large, avoidable costs in
human, social and economic terms. Of
the 57 million deaths that occurred globally in 2008, 36 million –
almost two thirds – were due to NCDs, comprising mainly cardiovascular
diseases, cancers, diabetes and chronic lung diseases. The combined
burden of these diseases is rising fastest among lower-income countries,
populations and communities, where they impose large, avoidable costs in
human, social and economic terms.
NCD related deaths
About one fourth of global NCD-related deaths take place before the
age of 60. NCDs are caused, to a large extent, by four behavioral risk
factors that are pervasive aspects
of economic transition, rapid urbanization and 21st-century life:
tobacco use, unhealthy diet, insufficient physical activity and the
harmful use of alcohol. The greatest effects of these risk factors fall
increasingly on low and middle-income countries, and on poorer people
within all countries, mirroring the underlying socioeconomic
determinants.
Among these populations, a vicious circle may ensue: poverty exposes
people to behavioural risk factors for NCDs and, in turn, the resulting
NCDs may become an important driver to the downward spiral that leads
families towards poverty.
As a result, unless the NCD epidemic is aggressively confronted in
the most heavily affected countries and communities, the mounting impact
of NCDs will continue and the global goal of reducing poverty will be
undermined.
A major reduction in the burden of NCDs will come from
population-wide interventions, which are cost effective and may even be
revenue-generating, as is the case with tobacco and alcohol tax
increases, for instance. But effective interventions, such as tobacco
control measures and salt reduction, are not implemented on a wide scale
because of inadequate political commitment, insufficient engagement of
non-health sectors, lack of resources, vested interests of critical
constituencies, and limited engagement of key stakeholders. For example,
less than 10 percent of the world’s population is fully protected by any
of the tobacco demand-reduction measures contained in the WHO Framework
Convention on Tobacco Control.
Improved healthcare, early detection and timely treatment is another
effective approach for reducing the impact of NCDs. However, appropriate
care for people with NCDs is lacking in many settings, and access to
essential technologies and medicines is limited, particularly in low and
middle-income countries and populations.
Many NCD-related healthcare interventions are cost effective,
especially compared to costly procedures that may be necessary when
detection and treatment are late and the patient reaches advanced stages
of disease. Health systems need to be further strengthened to deliver an
effective, realistic and affordable package of interventions and
services for people with NCDs.
As the magnitude of the NCD epidemic continues to accelerate, the
pressing need for stronger and more focused international and country
responses is increasingly recognized by Member States. Much has been
learnt about the causes, prevention and treatment of NCDs over the past
three decades, as important achievements have been made in reducing
mortality in many high income countries; the evidence base for action is
steadily mounting and global attention to the NCD epidemic is
intensifying. Non-communicable diseases include: cancer, cardiovascular
disease, chronic respiratory disease and diabetes. Tobacco use,
unhealthy diet and physical inactivity are responsible for the vast
majority of death and disability caused by NCDs. These threats have
increased dramatically with recent global changes such as globalization
and urbanization, and related demographic, economic and technological
developments. Urbanization, employment patterns, social trends and mass
communication work together to create an environment that restricts
choices and shapes the behaviours that influence health, including
quality of diet and level of physical activity. In extremely low income
countries, many NCDs are linked to infections. These include rheumatic
heart disease, cervical cancer, liver cancer and stomach cancer.
NCDs affect men, women and children of all social and economic
levels. The large majority of those suffering from NCDs live in low and
middle-income countries. In high-income settings, NCDs are most common
among the poor. Poverty is both a cause and a consequence of NCDs.
Limited access to healthcare, insurance and/or social benefits in
low-income countries means that the death or disability of a breadwinner
often impoverishes an extended family. The loss of productivity of
workers killed or disabled by NCDs is enormous and it threatens to
undermine the economic growth of many developing and emerging economies.
NCDs impede progress toward the Millennium Development Goals, especially
those on factors affecting health like poverty and education.
Many people still believe that NCDs primarily affect the wealthy.
NCDs are seldom seen to be a health priority in low and middle-income
countries. Because the behaviours that contribute so heavily to NCD risk
are shaped by policy, norms and environmental factors, solutions require
the commitment and collaboration of many sectors that are not accustomed
to taking health needs into account.
Governments, civil society and elements of the private sector are
beginning to recognize that we must invest in NCD prevention to protect
socio-economic development. Policymakers, educators, healthcare
providers, corporations, municipal authorities, the media and others are
starting to work together to raise the priority given to
non-communicable diseases, to increase resources allotted to them and to
move people to action. Effective tobacco control policies, changes in
food content, guidelines and policy on labelling and marketing, plus
city planning that facilitates active (as opposed to motorized)
transport are among the measures that will help get the NCD epidemic
under control.
The UN Summit on NCDs, to be held in September 2011, will call on
heads of State to fully recognize the burden imposed by NCDs and to show
concrete commitment to overcoming it.
Laser treatment unit for prostate
The first Laser treatment unit for prostate gland was installed at
Nawaloka Hospitals recently.
Prostate gland enlargement affects up to 43 percent of men over the
age of 60, leading cause of voiding difficulties, half of all men over
50 have prostate gland enlargement symptoms the percentage growing to 80
percent of men over 80. Prostate gland is a walnut sized cone shaped
organ situated just below the urinary bladder and the urine passes
through it.
At young reproductive ages the gland contributes to the production of
semen and provide nutrients to the sperms thus forming an essential part
of male reproductive systemic. However with ageing specially after 45
the central core of the gland undergoes certain changes (benign
prostatic hypertrophy-BPH) making the gland to swell in size. This newly
formed tissue can block the urethra or the urine pipe causing symptoms
such as difficulty in starting the stream, straining to pass urine,
stopping and starting urinary flow, getting up in the night to pass
urine and sometimes total blockage which is called acute urinary
retention.
Although can often be handled adequately with medical treatment,
patients who continue to have significant voiding problems will
eventually require surgical intervention, to avoid long-term sequeale
such as urinary retention, urinary track infections diverticula and
bladder calculi. When surgical treatment was considered the traditional
only surgical option was to open the abdomen and core out the enlarged
gland which was associated with many complications such as bleeding,
wound infection, pain, prolonged hospitalization and delayed return to
normal daily pursuits.
Fortunately over the last few decades surgery through telescopic
instruments introduced through the urinary passage and electrical
cutting of the gland (Trans urethral resection of the prostate - TURP)
has nearly replaced the open surgery. Alternate therapies have been
developed in an attempt not only to provide a surgical treatment for
prostate gland enlargement but also to minimize the risk of post
operative complications and the length of hospital stay.
“Latest laser method (Holmium laser) which has overcome most of these
problems has been introduced to Sri Lanka by Nawaloka Hospitals PLC by
its recently acquired Versa Pulse Power Suite 100 Watts Holmium Surgical
Laser for urological applications, which was launched on June 18, 2011.
Holmium laser prostate surgery will be relatively more economical to the
patient as many patients can be operated with a single laser fibre and
this method can be used not only for evaporation but also to cutoff
large glands more completely without bleeding, avoiding re-operations.
Even very large prostates which will need open operations could be
removed with this new Laser,” a spokesman for Nawaloka Hospitals said.
“The new laser for the prostate has cost nearly 17 million SLR in
addition to the supportive endoscopic instruments which cost nearly 10
million. In spite of these heavy capital expenditure Nawaloka Hospitals
PLC has made plans to maintain the services at a viable and affordable
financial level.”
It will be either on par or much more economical than the available
older resection methods and laser methods.
A trained Local senior Urological surgeon and a team performed the
surgery following a live demonstration and instructional work shop
conducted on June 18-19, 2011 by Dr Anil Varshney from India, who is a
regional expert on this new Holmium laser prostate surgery, in
collaboration with the Sri Lanka association of urological Surgeons,” he
added.
Art of Clinical Medicine
Title: Art of clinical
medicine
Author: Dr S D K Perera,
MD, FRCP (Consultant Physician and Gastroenterologist)
This short text book provides a practical account of Clinical
Medicine. It focuses on the interpretation of history, physical
examination and relevant investigations that are required to make a
correct diagnosis.
This is a 264 page book with 277 colour photos.
CD is provided.
This book is suitable for undergraduates, postgraduates and also for
those who are preparing for ERPM examination.
Distributors - Samayawardana Books, Maradana. |












")

